A Packet of Paper Is Not a Community

Photo by Mike van Schoonderwalt from Pexels I remember the moment clearly because it felt fundamentally wrong. A close friend had just been discharged from the hospital. He was not truly better, only stable enough to leave. A nurse gave her a packet of papers, reviewed a few instructions, and wished her well. She was sent home without anyone asking if she had support or how she would manage the challenges awaiting her outside the hospital. And there was a lot waiting. Medications she didn’t fully understand. Follow-up appointments, he wasn’t sure how to schedule. Symptoms she was told to monitor, but didn’t quite know how to interpret. She sat at her kitchen table later that evening, papers spread out in front of her, trying to make sense of it all. I sat across from her, realizing something I hadn’t fully put into words before: This wasn’t care. This was information. And information, by itself, isn’t enough. We often assume healthcare is comprehensive: once a patient sees a doctor, receives treatment, and is given instructions, the system’s job is complete. On paper, this may be true. In reality, the real work begins after discharge, when responsibility shifts entirely to the patient, often without the necessary support. The gap between what the system provides and what people actually need is where outcomes begin to deteriorate. Healing does not occur through discharge instructions alone. It takes place in daily life: when someone can access their medication, has support to attend appointments, understands their symptoms, and feels confident to act. Most importantly, it happens when they are not alone. But too often, they are. What I witnessed was not the failure of any individual provider, but a systemic issue. The system is designed for efficient clinical care, not for supporting patients after discharge. It assumes that once information is provided, it will be understood, remembered, and followed, and that patients have the time, resources, and stability to comply. This assumption is the root of the problem. A packet of paper cannot address the complexities of real life. It can’t account for the single parent who has to choose between going to a follow-up appointment and going to work. It can’t account for the patient who doesn’t have reliable transportation, or the one who doesn’t fully understand the medical language but is too overwhelmed to ask questions. It can’t account for fear, confusion, exhaustion, or the quiet moments when someone wonders if they’re doing any of this right. Most importantly, it cannot replace genuine support. That day changed my perspective. I realized the largest gaps in healthcare often exist outside the hospital, in homes and communities where individuals are expected to manage their health without a safety net. We frequently discuss access to care, but rarely address what happens after care is provided. We measure success by whether treatment was received, not by whether patients can follow through. We focus on the clinical encounter and overlook the factors that determine long-term outcomes. Sitting with my friend, I understood something I had not fully realized before: A discharge is not the end of care. It’s the beginning of responsibility. Responsibility without support is not a solution; it sets patients up for failure. To achieve better outcomes, we must think beyond appointments, hospitals, and paperwork. We need to ask a different question: What does someone need to succeed once they leave? Until we answer this, we are not building a true system of care. We are simply handing out instructions and hoping for the best.
Healthcare education is evolving. But not fast enough.

The American Association of Colleges of Nursing is calling for more connection, more engagement, and more belonging. This matters not just in classrooms—but in hospitals, clinics, and conversations between humans. They want to ensure that everyone experiences the nursing education “…with open doors, meaningful relationships, and a shared sense of purpose.” And this ideal makes sense for all healthcare students, doesn’t it? Years ago I was an Occupational Health Nurse at a manufacturing company. I was observing how poor communication and interpersonal dynamics were creating problems with situations involving employee injuries and illnesses. I was asked to present a workshop on listening to the management team. The problem was, I didn’t know how to teach a skill like listening. So, I did all the talking. :). No discussion. No practice experience. No reflections. No fun. It was not engaging, connecting, or effective. Since then, I’ve learned a lot about teaching communication-related skills and competencies. That’s where Medical Improv comes in. It’s a hands-on teaching modality that builds emotional intelligence, confidence, communication, and positive relationships. I’ve seen it over and over again! 💬 When 150+ students at Harper College participated in a 2.5-hour workshop, over 90% reported improved listening, feedback, and self-awareness skills. And in terms of engagement, just look at the faces and body language in this and more session photos. Professor Joyce Shaw, DPT, puts it plainly: “An asset for all instructors…easy to integrate, impactful for students.” Faculty, patients, and future healthcare workers: we are all part of this web. 👉 Learn more about the Medical Improv Toolkit: 3 Paths into Practice! here: Questions? Reach out: [email protected]
Medical Improv as a Way to Promote Dignity in Healthcare
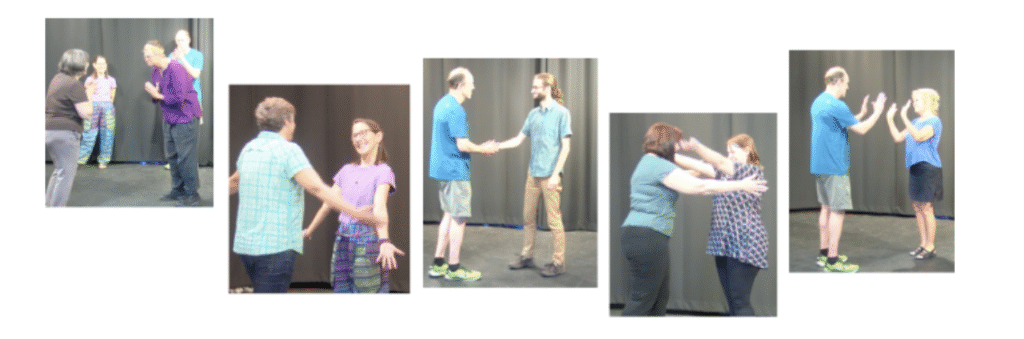
Experiential activities adapted from theatre education and improvisation are a form of Medical Improv. They become a part of this emerging field when used to address goals or outcomes we seek in healthcare. There are literally hundreds of experiential activities and variations that can be used to teach communication-related skills and improve healthcare outcomes. Critical outcomes such as patient safety, patient experience, workforce health and wellbeing and even cost-effectiveness. That’s because improving theses skills helps us become our best selves which impacts all of our relationships, are ability to work in teams and lead all of which in turn impact outcomes. Why Status Activities? One branch of activities developed by improvisation guru, Keith Johnstone refers to status activities. In theatre, these activities help actors make scenes more interesting for audiences. While Johnstone’s legendary book, Impro is directed towards actors, the chapter on ‘Status’ is fascinating for anyone interested in human behavior. In healthcare, status activities offer great opportunities to discuss dignity and hierarchy. Dignity for our patients, families, colleagues, and selves, healthy vs. toxic hierarchy, and their interrelationship. These activities, when facilitated properly, provide experiences where participants become more aware about how high/low status and dignity look, sound, and feel. This awareness then becomes a door to talking about our healthcare hierarchy in constructive ways while coming from a place of dignified interconnectedness! All in the spirit of mutual respect and co-creative problem-solving! Dignity Exchange My favorite activity is called Dignity Exchange, an activity created by Liz Korabek-Emerson, myself and our students. In short, with coaching, people walk around as if they are highly superior to everyone else. This is portrayed with body posture, facial expression, tone of voice, and an internalization of what it ‘feels’ like. From left to right: Susan Conboy, Robin Masia, Patricia Corso, John Klossner & Jody Fuller – Boynton Improv Education After they’ve spent a minute or so in high status, I invite them to shake it off. Then, with a similar process, they assume low status personas. This is followed with another invitation to “shake it off”. From left to right: Patrica Corso, Carolyn Vibbert, John Klossner, Glenna Kimball, Barbara Trimble, & Curran Russell – Boynton Improv Education It has always surprised me how little modeling or coaching people need to embody these ways of being. As if, somehow in our life experiences we know. Maybe we’ve been treated or treated others in such ways? Maybe both? And shaking it off can feel like a big relief! The coaching process now turns to language and modeling around self-respect and dignity. What does that look like? Sound like? Feel like? And people know this too! In general, it feels good! Once they embody a feeling of dignity, they pair up and face each other. One assumes high status while the other, low status. While facing each other and over the course of about a minute they switch status postures. Once that is done they are instructed to find the place where they feel dignity for themselves and each other. What happens next is incredibly inspiring and affirming for the best of humankind! Visceral Moments of Dignity These heartfelt moments between people are a privilege to witness. And as you can see in this pic, they show it in a variety of ways. It is, as if, we are tapping into a human quality that is already there. And in facilitating this activity we are reminded of what some of our best qualities are! From left to right: Liz Korabek-Emerson, Robin Masia, Beth Boynton, John Klossner, Lori Austin, Robin Masia, John Klossner, Curran Russell, Susan Conboy, Patrica Corso, John Klossner, & Glenna Kimball – Boynton Improv Education If you’d like to know more, please feel free to reach me: [email protected]. Also, this handout from an event with Human Dignity and Humiliation Studies a few years ago offers more guidance about teaching Dignity Exchange. And I happily invite you to explore a variety of Medical Improv resouces and the exciting new self-paced 3 Paths into practice!
6 Communication, culture, and leadership issues that ensure qualified staff
Having unqualified people in jobs they should not be in is not an issue about diversity, but rather one of communication, culture, and leadership. Here are six related issues that influence the likelihood that qualified staff are in positions that require high reliability: 1. Leaders and staff are skilled at giving and receiving constructive feedback so that teaching and learning are going on all the time. 2. All levels of staff are willing and able to ask for help, set limits, delegate tasks or say “No” when they need to. 3. All levels of staff are respectful of others’ limits, and leaders respectfully address patterns of excessive need for help, time management, and training needs on an individual by individual. Image by Ahmad Ardity from Pixabay 4. Expectations for performance are clear and consistent. 5. Leaders advocate for and ensure the resources necessary to follow protocols, procedures, and policies are available (incl: staff, time, money, training, and equipment). 6. Evaluations of performance are objective, fair, respectful, and intended to ensure high reliability. Identifying underperforming or unqualified people need not be a personal affront and can include support in finding an appropriate job match. Can you think of any other issues as viewed from this lens?